Knee Anatomy
Knee pain caused by arthritis, injury, or joint degeneration can severely affect mobility and quality of life. When conservative treatments such as medications, physiotherapy, or injections no longer provide relief, knee replacement surgery may be the most effective solution. Patients looking for a knee replacement surgeon in Jaipur often consult Dr. Amit Meena , a fellowship-trained orthopedic specialist known for advanced joint replacement procedures and patient-focused care.
Dr. Amit Meena specializes in partial knee replacement surgery, total knee replacement, and bilateral knee replacement surgery using modern surgical techniques and high-quality implants. With extensive experience in treating complex knee conditions, he helps patients regain mobility, reduce chronic pain, and return to an active lifestyle.
For patients whose joint damage is limited to a specific part of the knee, partial knee replacement surgery may be recommended. This procedure replaces only the damaged section of the joint, preserving healthy bone and ligaments while allowing faster recovery. In cases where both knees are severely damaged due to arthritis or injury, bilateral knee replacement surgery may be performed to restore joint function and stability.
Choosing the best knee implants in India is an important part of successful knee replacement surgery. Dr. Amit Meena uses advanced and internationally approved implants designed for durability, improved joint movement, and long-term performance. His personalized treatment approach ensures that each patient receives the most suitable surgical option based on their condition and lifestyle.
Patients searching for the best knee doctor or top orthopedic doctors in India. Dr. Amit Meena’s experience in knee replacement and sports injury treatment. His focus on modern surgical methods, proper rehabilitation, and long-term joint health helps patients achieve better outcomes after surgery.
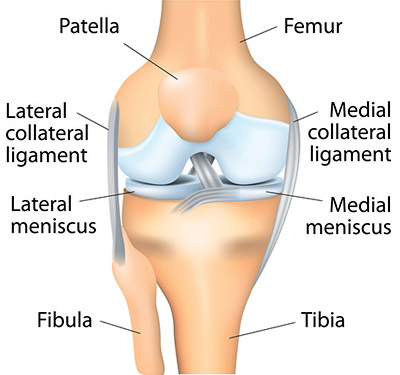
The knee joint, which looks like a simple hinge joint, is actually one of the most complex joints in the body. It consists of the femur (thighbone), tibia (shinbone) and patella (kneecap).
The knee is a synovial joint, which means it has a lining called synovium. This lining produces a fluid that helps to lubricate and provide nutrients to the inside of the joint.
Articular cartilage is the smooth tissue covering the ends of the femur and tibia. Damage to this cartilage is a common cause of arthritis.
Skeletal Anatomy
Femur
The femur (thighbone) is the largest and strongest bone in the body is the weight-bearing bone located in the thigh. It serves as the main attachment point for most of the muscles in the knee area.
Condyle
The two femoral condyles make up for the rounded end of femur. Its smooth articular surface allows the femur to move easily over the tibial (shinbone) meniscus.
Tibia
The tibia, also known as the (shinbone), is the second largest bone in the body and serves as the main weight-bearing bone of the leg. The menisci partially cover the top part of the tibia where it connects with the femur. The menisci function as shock absorbers, helping to protect the smooth surface of the shinbone and also supporting the twisting movements of the knee.
Fibula
The fibula, which is not a bone that supports the body's weight, serves as a point where the Lateral Collateral Ligaments (LCL) and the biceps femoris tendon attach. The joint between the tibia and fibula allows for a small amount of movement, contributing to some flexibility as a result of the muscles connected to the fibula acting upon it.
Patella
The patella, also known as the kneecap, is connected above to the quadriceps tendon and below to the patellar ligament. It sits against the front part of the lower end of the femur, providing protection to the knee joint. The patella functions as a pivot point for the quadriceps muscle, keeping the quadriceps tendon elevated from the lower part of the femur.
Menisci
The medial and lateral menisci are thin, C-shaped fibrocartilage structures that partially cover the tibial surface where it meets the femur. Most of the meniscus does not have a blood supply, which means it cannot heal naturally like other tissues in the body when it gets injured. With age, the meniscus tends to wear down and can develop degenerative tears. When the meniscus is damaged, the torn parts may move abnormally within the joint. The menisci serve as shock absorbers, helping to protect the tibial articular surface and supporting the knee's rotational movement. As secondary stabilizers, the menisci work along with the ligaments to help keep the knee stable, and they perform most effectively when the surrounding ligaments are in good condition and not damaged.
Soft Tissue Anatomy
Anterior Cruciate Ligament (ACL)
The anterior cruciate ligament (ACL) is the main ligament that helps keep the knee stable. It is positioned in the middle of the knee joint and connects the femur, which is the thigh bone, to the tibia, which is the shin bone, passing through the center of the knee. The ACL stops the femur from moving backward over the tibia, or the tibia from moving forward over the femur. Along with the posterior cruciate ligament (PCL), the ACL helps stabilize the knee by preventing it from rotating improperly. If either of these ligaments is badly injured, the knee may feel unstable when the person plants their foot or turns their body, leading to the knee giving way or buckling.
Posterior Cruciate Ligament (PCL)
Less research has been conducted on the posterior cruciate ligament (PCL) because it is less commonly injured compared to the anterior cruciate ligament (ACL). The PCL stops the femur from sliding too far forward over the tibia. It serves as the primary stabilizer of the knee and is almost twice as strong as the ACL. This ligament also plays a key role in keeping the knee properly rotated in the center.
Collateral ligaments
Collateral Ligaments prevent hyperextension, adduction, and abduction.
ü Superficial MCL (Medial Collateral Ligament) connects the medial (inner) epicondyle of the femur to the medial condyle of the tibia and resists valgus (bending out) force.
ü Deep MCL (Medial Collateral Ligament) connects the medial (inner) epicondyle of the femur with the medial meniscus.
ü LCL (Lateral Collateral Ligament), entirely separate from the articular capsule, connects the lateral (outer) epicondyle of the femur to the head of the fibula and resists varus (bending in) force.
Biomechanics of the Knee
The knee joint is a type of hinge joint that has developed to perform specific functions. The primary actions it can perform include bending (flexion), straightening (extension), turning inward (medial rotation), and turning outward (lateral rotation).
Flexion
When the knee is bent, the cruciate ligament becomes tight, while the collateral ligaments are loose. Maximum flexion of the knee is 120-150 degrees.
Extension
When the knee is extended or straightened, the lateral and medial collateral ligaments as well as the ACL are taut. Maximum extension of the knee is 5-10 degrees.
Medial Rotation
This movement can only be performed when the knee is bent. The cruciate ligaments allow the tibia to rotate inward by twisting around each other, which makes this movement possible. Maximum internal rotation is 30-40 degrees.
Lateral Rotation
Lateral rotation is possible only when the knee is flexed. The cruciate ligaments control lateral rotation of the tibia by untwisting around each other to enable this movement. Maximum external rotation is 30-40 degrees.